


Is happiness really that simple?
Sure, it's easy to say, "Think positively." But to actually do it? Not so much.1 We spend bazillions of dollars trying to buy happiness and yet somehow we're not satisfied.2 I don't have any money left to spend, so my options are (a) a life of misery and despair, or (b) find a cheaper alternative.
The Coldplay Proof, and searching the InterGoogle
Socrates asserted that the highest good for any human being is happiness.3
 If given that x = highest good, and y = best things in life, the equation derived from Coldplay's 2005 album X&Y clearly delineates that the highest good and best things in life are considered conjoined.4 And as we all know that the best things in life are free, we can safely apply this adage to the highest good, which was previously equated with happiness. Therefore, happiness = free. QED.
If given that x = highest good, and y = best things in life, the equation derived from Coldplay's 2005 album X&Y clearly delineates that the highest good and best things in life are considered conjoined.4 And as we all know that the best things in life are free, we can safely apply this adage to the highest good, which was previously equated with happiness. Therefore, happiness = free. QED.With my Coldplay proof in mind, I thought about the various options at my disposal. I am not 65 years old so I don't qualify for Medicare, and I do not qualify for Medicaid. This greatly reduces my chances of free drugs.5 There are prescription assistance programs out there, but that sounds like a lot of effort, and I'd have to go to a physician, and frankly I'm just looking to exert the least amount of effort. So, pills are out.
 I considered the sugar daddy route - a handsome silver fox, showering me with gifts and money. But two obstacles: one, my husband would likely not care for this option (unless I scored some free swag for him too, namely beer and hockey tickets, but I'd want those too so we'd have to grudge match. We don't own any ridiculous spandex costumes to engage in said match, so the point is moot.). Two, the Coldplay proof works on the assumption that the best things in life are free, so any money spent on gifts by said sugar daddy (or the money itself, presumably garnered in some shady overseas "consulting" job) would automatically render gifts and money not the best things in life. Two down: pills and sugar daddy are out.
I considered the sugar daddy route - a handsome silver fox, showering me with gifts and money. But two obstacles: one, my husband would likely not care for this option (unless I scored some free swag for him too, namely beer and hockey tickets, but I'd want those too so we'd have to grudge match. We don't own any ridiculous spandex costumes to engage in said match, so the point is moot.). Two, the Coldplay proof works on the assumption that the best things in life are free, so any money spent on gifts by said sugar daddy (or the money itself, presumably garnered in some shady overseas "consulting" job) would automatically render gifts and money not the best things in life. Two down: pills and sugar daddy are out.All right, time to hit the InterGoogle for some ideas. Key words: free, happiness.6 The resulting hits were essentially fluff, self-help rainbows and butterflies, and snake oil salesmen (including one called Real Hot Lava that advertised "free happiness on sale today." Hmm.).
Since the magical solution had not appeared before my eyes, I figured I may as well fall back on that expensive education I received, which included a number of classes in psychology, and flicked the dredging switch in my brain to "on."
"A Freudian slip is when you mean one thing, but you say your mother."
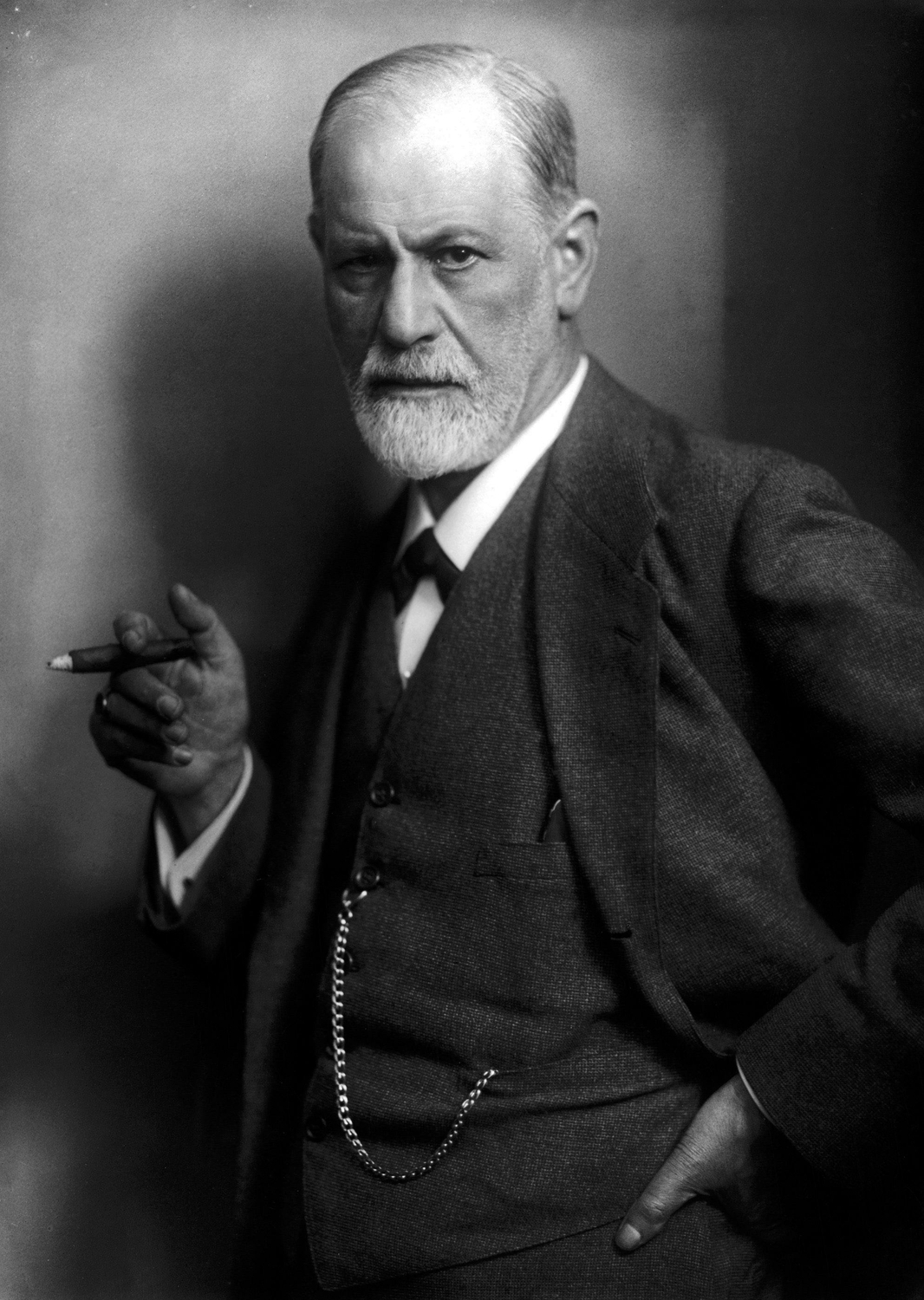
Sigmund Freud was an Austrian neurologist who created the clinical practice psychoanalysis. He is best known for his theories of the unconscious mind (ego, super-ego and id), dream analysis, free association, and a little-known theory he called the Oedipus complex.7
His work in the late 1800s / early 1900s defined and dominated psychotherapy for almost half a century, but there wasn't much in the way of rigorous scientific study into the efficacy of psychoanalysis. In fact, the rule of thumb was that about a third of patients got better, a third got worse, and a third stayed the same.
 The popular theory of depression at the time was psychodynamic - a theory of inner conflicts which surface in behavior or emotions. In other words, people were depressed because of "inverted hostility." Freud said that a depressive was angry at someone else (e.g. mom or dad), but turned the hostility inward. The unconscious rejected this anger, knowing it wasn't logical, blocked the anger from entering the consciousness, and returned inward again. The depressive was consumed with unconscious rage, which manifested in depression. Freud hypothesized that digging up the original reasons behind the anger and dealing with them could alleviate the rage.
The popular theory of depression at the time was psychodynamic - a theory of inner conflicts which surface in behavior or emotions. In other words, people were depressed because of "inverted hostility." Freud said that a depressive was angry at someone else (e.g. mom or dad), but turned the hostility inward. The unconscious rejected this anger, knowing it wasn't logical, blocked the anger from entering the consciousness, and returned inward again. The depressive was consumed with unconscious rage, which manifested in depression. Freud hypothesized that digging up the original reasons behind the anger and dealing with them could alleviate the rage.This took a long time. Years. And there weren't randomized clinical trials to unequivocally prove that the therapy even worked. The psychoanalysts benefited financially, but according to the rule of thumb stated above, two thirds of the patients didn't improve.
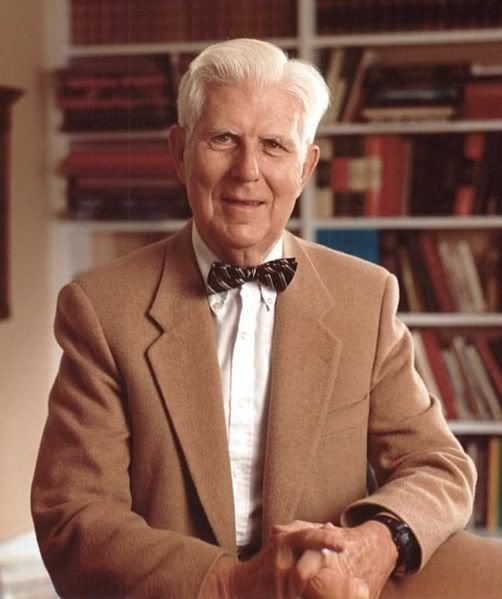
Fast forward to the 1960s, a time of counter-culture and social revolution. A psychiatrist named Aaron Beck was quietly working on his own revolution within the field, work that is now "the most well-funded, deeply researched, popular and rapidly growing" form of psychotherapy across the globe.8
The Beckian revolution
Aaron Temkin Beck is an 88-year-old practicing psychiatrist living northwest of Philadelphia, and looks like the kind of guy you'd want for a grandpa - kindly, pastoral, maybe a bit mischievous.
 In particular, one patient's notes from his archives stick out. Not
In particular, one patient's notes from his archives stick out. Notbecause the patient was all that unusual, but because of how that
patient contributed to Beck's seminal work in developing Cognitive
Behavior Therapy.
The earliest notes from the patient's file date from the 1960s - a man "in his mid-40s, good career, loving wife, four beautiful children, and trove of close friends. Privately, however, he struggled with an acute tendency toward self-criticism. He was of the type that can't help but interpret neutral events as harsh reflections on his personal worth. He was forever searching for approval, and forever anticipating disapproval."
Keep this patient in mind as we travel back in time to explore Beck's curriculum vitae. Beck graduated from Yale Medical School in 1946 and specialized in neurology after graduation. He was attracted to neurology because the discipline was "exact" - he was very much a believer in the scientific method and empirical study. Yet the hospital to which he was assigned had a shortage of psychiatry residents, so he had to do a six-month rotation in that field. Psychoanalysis was "soft-minded and esoteric, more a faith than a medical discipline," but the mystique was also appealing, so Beck stuck with it. When he questioned whether psychoanalytic interpretations "had evidence to back them up, his friends suggested that unconscious resistances were preventing him from realizing the truth."
Beck wanted to prove that psychoanalysis was valid, using experimental evidence, but he had no training in research nor previous rigorous scientific studies of psychoanalysis to fall back on, so he asked academic scientists at Penn (where he was working) for help in experimental design.
Surprisingly, or perhaps not, his first trial failed miserably. Beck theorized that Freud's inverted hostility theory could be proven by scrutinizing the content of patients' dreams. He compared depressive patients' dreams to dreams of patients who were not depressed. The depressed patients' dreams were not full of hostility; in fact, "they were less hate-filled than the dreams of the non-depressed." What he found instead in those dreams were deprivation, disappointment, hopelessness - what they were feeling in their daily lives. Since he couldn't find the hostility in their dreams, perhaps it was buried much deeper in the depressed patients' psyche than previously thought.
Two cracks in the shell
Thankfully his scientist colleagues told him that all he had proven was that depressed patients were depressed. Not exactly earth-shattering news. Beck tried again - this time, he tested the hypothesis that depressives would "actively court unpleasant experiences" - a kind of masochistic need for suffering. "A researcher subtly expressed approval and disapproval based on the types of words a patient chose from a multiple-choice questionnaire," and at the end Beck found that patients "seemed to hunger for improvement." This was the "first crack in the shell."
The second crack "split everything wide open," and came about during a patient's therapy session. A "promiscuous young women" he had been treating for more than a year spent her sessions "describing her lurid sexual encounters in great detail while Beck sat impassively in a chair behind her, taking notes."
At the end of the session, Beck asked the patient, "How do you feel?" - a normal question for a session.
"Very anxious, doctor," she replied. Of course, Beck told her. That was because she was being forced to confront her deepest sexual impulses [which was in line with Freud's psychodynamic theory]. When these impulses rose to her consciousness, breaking through her ego's defense systems, they caused anxiety.Beck found that by focusing on this new theory, he could alleviate symptoms in as few as 10 sessions, and the progress stuck. "I concluded that psychoanalysis was a faith-based therapy," he has said, "and that if I was going to practice or teach therapy, it had to be empirically driven."
"You're right," she said. "That's brilliant." But she sounded tentative. Beck told her so. "Actually, she said, "I was afraid I was boring you."9 Beck was surprised. Fear of boring one's analyst is not uncommon, but this patient had never mentioned it before. He asked her how often she thought she was boring.
"Oh, all the time," she said. "I think it when I'm here with you, and I think it when I'm with everyone else." This was nothing short of revelatory. As engaging as his patients' monologues could be, and as much emphasis as analytic doctrine placed on them, it was their mundane, reflexive, almost forgotten thoughts that now seemed to hold the true explanatory power. ... Once Beck realized this, he began to uncover similar thoughts in all his patients, as well as in his friends, his family, and himself. Our daily lives, he concluded, unwind to the accompaniment of a quiet but constant self-talk, through which all external events are filtered.
Cognitive Behavior Therapy
Remember the patient described above? Had what appeared to be a happy life, but interpreted neutral events as harsh reflections on his personal worth? That patient was "none other than Beck himself."
Out of all these collected insights and experiments, Beck developed Cognitive Therapy, "whose guiding principle is that the driving forces of mental dysfunction are habitual, unrealistic, self-defeating ideas."
 CT drops the endless search for past hurts, teaches patients how to prevent negative thoughts from creeping into their minds and coaches them on how to cope. "We are starting to believe that what you think
CT drops the endless search for past hurts, teaches patients how to prevent negative thoughts from creeping into their minds and coaches them on how to cope. "We are starting to believe that what you thinkhas a powerful influence on symptoms," says Harvard psychiatrist Arthur Barsky in an excellent Forbes article on CBT.
Beck thought if you replace the bad thoughts with better, more realistic ones and happier emotions would follow. Since our thoughts cause our feelings and behaviors, not external things like people or situations, if we change the way we think we can feel better even if the situation doesn't change. What propelled CT forward, the Forbes article says, was the addition of behavioral techniques pursued by "psychologists rebelling against Freud ... including relaxation breathing exercises and exposure therapy for panic attacks. The two methods began merging in the 1970s to form cognitive behavioral therapy. The first mention of it in medical journals shows up in 1980." CBT is an umbrella term for a number of therapy approaches: rational emotive behavior therapy, rational behavior therapy, rational living therapy, cognitive therapy, and dialectic behavior therapy. (The National Association of Cognitive-Behavioral Therapists site has a nice overview here.)
Since those early days, CBT has been widely studied in clinical trials. The evidence is mostly in favor of CBT, in that it is either superior or at least non-inferior to pharmacological therapy (e.g. Prozac), and patients don't relapse as often as they do on pills. Not only can you avoid pills and their side effects, or supplement pills with CBT, but it's of short duration and evidence-based. There is even evidence to suggest that CBT modifies your neural circuitry. It is a first treatment of choice in many cases and is widely supported around the globe, and is spurring support for empirically-based therapies.
The UK's National Institute for Health and Clinical Excellence is spending $300 million to train and employ an additional 3,600 additional psychotherapists, primarily in CBT. In the U.S., Congress created and funded the National Child Trauma Stress Network (with more than $30 million per year) to disseminate empirically supported therapies to traumatized children and their families. CBT is the "cornerstone" of a new $117 million program to foster mental resiliency in soldiers (implemented by the U.S. Army), and since 2005 "the Veterans Administration has allocated more than $250 million per year to train therapists in empirically-supported therapies to cope with the influx of traumatized veterans returning from Iraq and Afghanistan. All of these programs highlight CBT" and Beckian-inspired methods.
 Now, CBT isn't perfect - a therapist needs to be properly trained in the method. And not everyone is a CBT convert. There are critics - a particularly vocal one that pops up often is Andrew Samuels, a psychotherapist and professor at the University of Essex.10 He makes the point that just because there is more evidence for CBT (in depression) than other therapies doesn't mean it is more effective. It means that the research on the other therapies has not been done.11 He also says that funding has helped researchers studying CBT so of course it has more evidence.
Now, CBT isn't perfect - a therapist needs to be properly trained in the method. And not everyone is a CBT convert. There are critics - a particularly vocal one that pops up often is Andrew Samuels, a psychotherapist and professor at the University of Essex.10 He makes the point that just because there is more evidence for CBT (in depression) than other therapies doesn't mean it is more effective. It means that the research on the other therapies has not been done.11 He also says that funding has helped researchers studying CBT so of course it has more evidence.While I understand his point, I think it's hogwash. Research on therapies has not been done, or at least not rigorously. That doesn't mean that CBT isn't effective, it just means that research on therapies hasn't been done. And yes, funded research will get done more than unfunded research, and naturally completed research will have more evidence than uncompleted research. This seems rather obvious and silly to state.
Samuels also says, "What you're witnessing is a coup, a power play by a community that has suddenly found itself on the brink of corralling an enormous amount of money. Science isn't the appropriate perspective from which to look at emotional difficulties. Everyone has been seduced by CBT's apparent cheapness."
I take issue with his statement that science isn't the appropriate perspective from which to look at emotional difficulties. Why not? The major thrust behind CBT's "coup" is the rigorous, scientific, data-driven approach. If this isn't a good way to look at emotional difficulties, what is? And if I can get equal or better outcomes from a short-term, cheaper therapy than a long-term, more expensive one, why wouldn't I go for the former?
Filling out the worksheet
You can find tools for CBT online, and they're quite easy to use. (I'm not saying you should use this in place of going to a trained psychiatrist, but if you want to see what the therapy is all about, it's interesting to check these out.) A simple and quick overview of CBT is provided by Specialty Behavioral Health here.
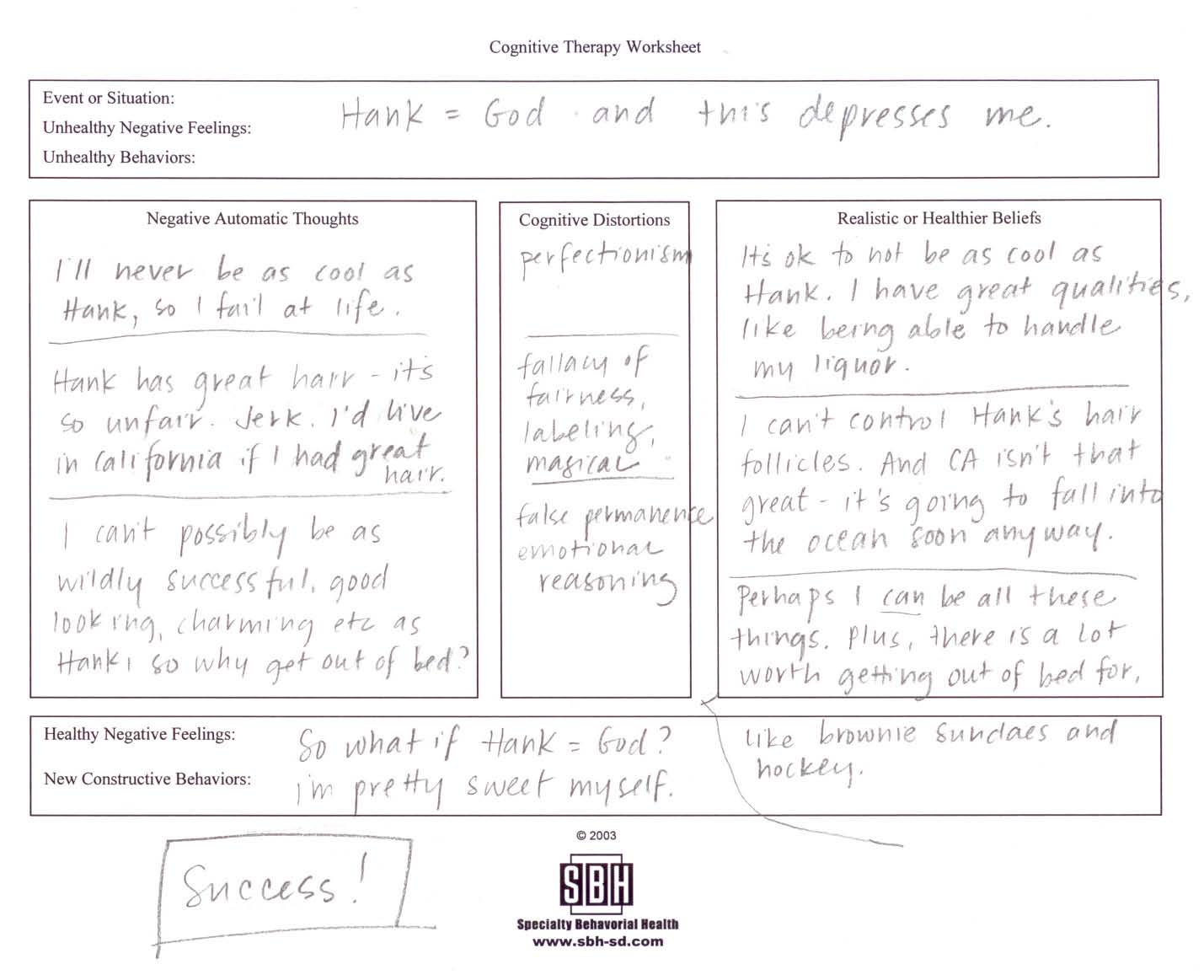
A standard three-column worksheet (click here) allows you to fill in negative thoughts, the cognitive distortions that supply those thoughts, and then the realistic or healthier beliefs.
In the first column, you fill in unhealthy negative thoughts. You can either write them directly in or use a daily mood and thought record (for example, here). In the second column, cognitive distortions related to thought patterns that keep us stuck in self-defeating patters (for example, here). Once you've identified the distortions, you can examine them and use prompts to change your thoughts to become more realistic or healthy (for example, here).
Say you're trying to finish your dissertation, but you're having trouble being positive and staying on top of things. Here is an example of how a person might fill in a worksheet and how the negative thoughts about completing the dissertation are turned into realistic, healthy, and productive thoughts.
I wanted to get the full experience, so I filled out a worksheet about something that depresses me:
What's next?
The corollary to Beck's data-driven methods is that other data could come along and supplant CBT. "Science is progressive, and already there is evidence to suggest that there may be more effective ways to treat mental illness than by scrutinizing thoughts." A trial in 2006, for example, suggested that in CBT "it is not the evaluation of thoughts but the changing of behavior that is doing the real therapeutic work."
Although a "mountain of evidence will need to be gathered before CBT's empirical altitude can be matched," Beck would likely not stand in the way if evidence supported another theory. Another researcher says of Beck, "He'd be the first person to put forth his theory and encourage that it be adopted, but he's always accepted other people's attempts to innovate. If, in fact, they could support their ideas with data."
For more on Beck, including information on self-report measures like the heavily utilized Beck Depression Inventory, check out The Beck Institute. Also, if you're interested, check out Beck's article in the American Journal of Psychiatry, "The Evolution of the Cognitive Model of Depression and its Neurobiological Correlates". For more handouts, check here and here.
1 There are a lot of distractions out there. To wit: I just realized that I had been staring at that Dance Dance Revolution ad at the top of my screen; it mesmerized me unconsciously and I zoned out. Three sentences in to the article and I'm already distracted. Not good. This is going to take a while, methinks. I scrolled down so I couldn't see the ad bar anymore; that should help.
2 $1.618 bazillion, to be exact, according to the most recent official numbers from the Commerce Department. Bazillion = a lot.
3 He also said the unexamined life is not worth living, thus predicting the rise of psychotherapy thousands of years before Freud was born. Seriously, did this guy know everything?
4 The X&Y album cover, although inspired by Baudot code, looks suspiciously like chromosomes. And the previous album, 2002's A Rush of Blood to the Head, included the song "The Scientist." Coincidence? Yeah, probably.
5 I could move to Las Vegas and win gainful employment as a prostitute, and demand I am compensated with free drugs. But if drugs are a form of compensation then they're not really free, ergo I am back to square 1.
6 I do not suggest using boolean searching with Google Search. "Free, happiness, NOT sugar daddy, NOT happy pills" turned up sites that were not in my target parameters.
7 Name this movie: "Hello. I'm Dr. Freud, but you may call me Siggy." Fun Freud Fact: he was an avid proponent and user of cocaine. Explains quite a bit.
8 All quotes that are unattributed by footnotes come from Daniel B. Smith's article, "The Doctor Is IN," from the Autumn 2009 issue of American Scholar, pages 20-31. Smith's article was the inspiration for this post. Click here to read the article.
9 Lurid sexual encounters described in detail? Boring? The billions of dollars the porn industry takes in every year seems to contradict this patient's belief.
10 I don't know much about Samuels, but he seems to be the go-to guy when reporters want to present the contrary opinion. Not that this lends credence to his claims; I'm just including him so you get the full picture.
11 http://www.independent.co.uk/life-style/health-and-families/health-news/the-big-question-can-cognitive-behavioural-therapy-help-people-with-eating-disorders-1128229.html




Comments