


What about quarantine?
A new review hopes to shed some light but because the review is primary of modeling papers - many of which looked like estimates and some more like guestimates - it may be only partially useful from an applied health policy perspective. The real answers may not be known for years.
With no vaccines and proposed medicines only now going into clinical trials, some U.S. states are being more heavy-handed than others. In dictatorships (Singapore, China) social authoritarianism is the norm and that has led to some calls to be more like them, while Sweden has been fine treating coronavirus like they do any other infectious respiratory disease, such as flu and has had no greater increase in deaths than they get from any other disease in vulnerable groups.
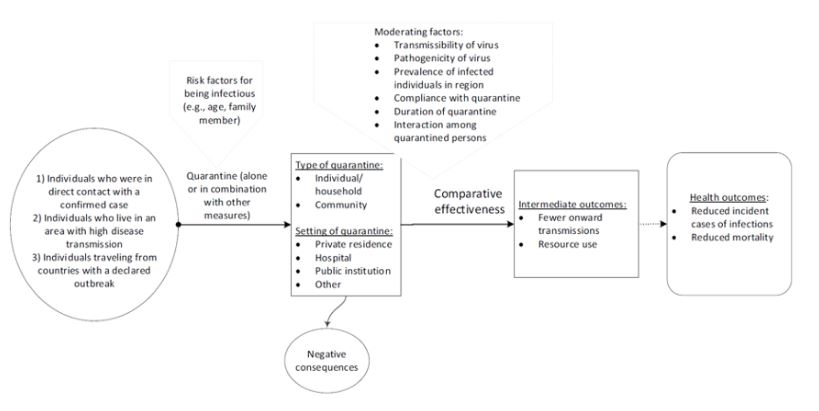
The analytical framework. Credit: 10.1002/14651858.CD013574
The authors concede confidence in the results is low despite narrowing their review down to 29 papers, some of which are retrospective cohorts, some are agent-based models, some stochastic, etc. but it is still good to have some parameters. The disease has real world consequences while papers based on food frequency questionnaires, magical claims of endocrine disruption homeopathy, and mouse studies do not. President Trump relied on a peer-reviewed paper to promote an off-label malaria treatment as a potential remedy and it was only after he mentioned the paper that it received the kind of peer review it would have gotten if peer review were really the gold standard that academics vying for government grants claim it is.
The authors only found 10 worthwhile papers trying to understand the impact of quarantine, school closures, etc. on SARS-CoV-2. The others were, for example, various previous flavors of coronavirus, SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome) and others.
They believe, qualifiers about validity aside, that quarantine of confirmed cases may avert high proportions of infections and deaths compared to doing nothing, which makes obvious sense, while benefit from quarantine of travelers just because they were from a country with a declared outbreak was small. Yet even that may not hold up once data replace numerical models. People may not have symptoms for 5 days so the risk from not putting any restrictions in place based on a simulated version of an outbreak is high.
The review authors believe their admittedly small sample of papers finds that quarantine plus school closures, travel restrictions, and physical distancing had a greater effect on the reduction of transmissions, and therefore critical care and deaths, than quarantine alone. So what the U.S. is doing is working.
Are we overdoing it? That is a topic for another article but those consequences also won't be known until the future.



Comments