


During the past two decades, China has been rapidly changing from a mostly agrarian environment of food production and consumption to a more urban environment typically found in Western industrialized societies.
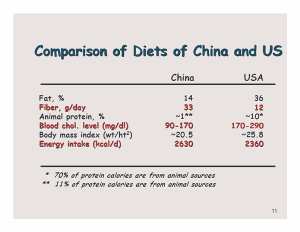
This means transitioning from a simple diet mainly comprised of a few locally-produced plant-based foods to a diet comprised of significantly more animal-based foods. Such a poor-to-rich transition leads to more food variety, more food availability (i.e., more calories), more total and animal-based protein and more total fat.
It also means less dietary fiber and antioxidants, almost exclusively found in plant-based foods. When transition opportunities arise in poor societies, there is a tendency to desire foods having nutritional characteristics typically found in rich Western industrialized societies in order to minimize or eradicate the diseases generally associated with poverty.
These 'diseases of poverty' are mostly infectious and communicable, like tuberculosis, pneumonia and parasitic diseases, among others. It has been well established that these diseases occur primarily because of poor sanitation and secondarily because of poor nutrition resulting from an inadequate consumption of calories (total food), protein and certain vitamin and mineral micronutrients.
Poor-to-rich dietary transitions generally emphasize four ideas, either intentionally or unintentionally. These include improved sanitation (especially to improve water quality), increased food availability, increased protein consumption (as with the development of a more productive livestock industry) and promotion of micronutrient supplementation (as with foods fortified with iodine and iron, for example).
As these dietary lifestyle transitions progress, however, it is not enough to consider only the health adversities of nutritional and health deficiencies typically found in rural, poor societies. The health diversities of a fully expressed transition also are of major importance. As diseases of poverty are minimized, for example, they are almost always replaced with so-called diseases of affluence. In poor-to-rich transitions, food becomes more available, varied and distributed, and sanitation conditions improve, each of which is highly desirable.
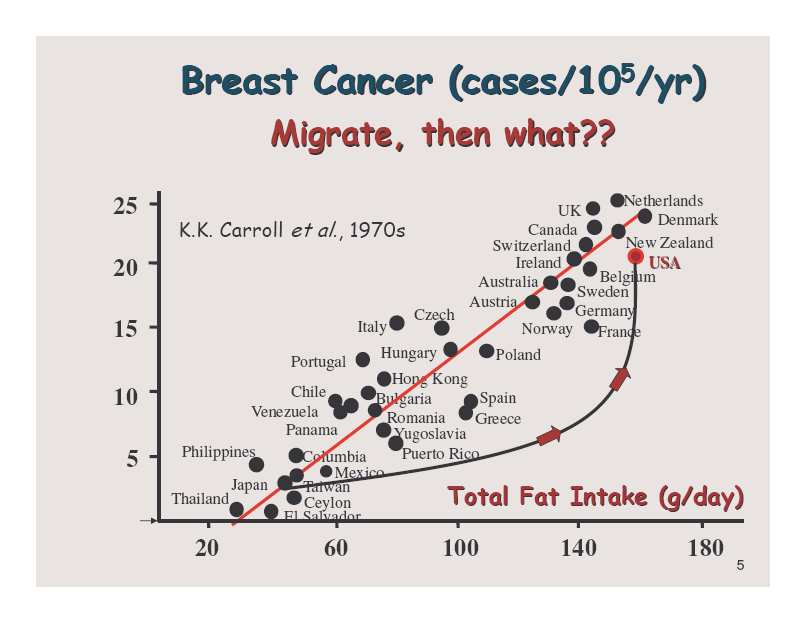
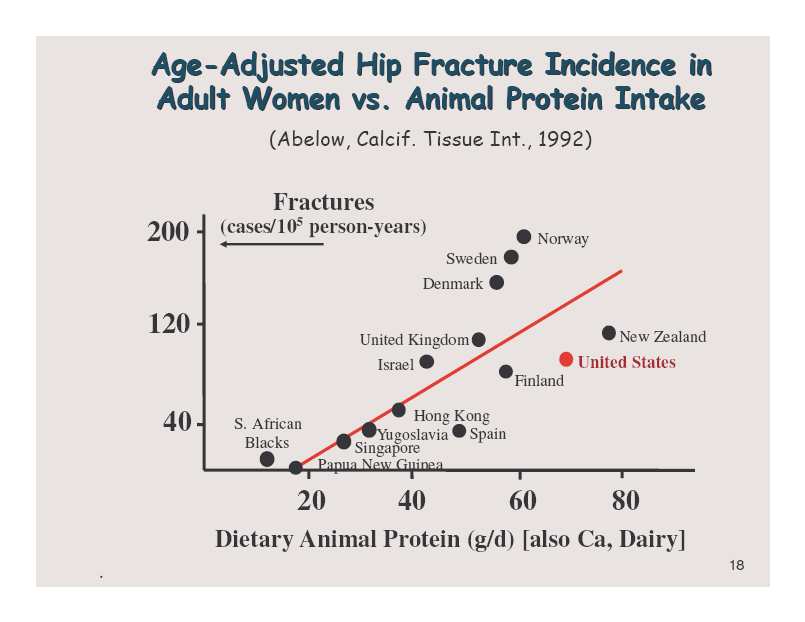
But there also are parallel increases in the consumption of animal-based foods and commercialized food products, This yields diets higher in total protein, animal-based protein, total fat, and refined carbohydrates (in place of complex carbohydrates), which leads to more ‘diseases of affluence’, as with age-dependent cardiovascular and neoplastic diseases among other metabolic disorders (e.g., obesity, diabetes, etc.)
Too often, however, there has been a tendency to oversimplify the causal links between diet and disease that emerge with these transitions, thus leading to public health programs and strategies that are unproductive. Attempts to correct micronutrient deficiencies, for example, are not supported with evidence of widespread benefit, with the possible exception of iron and iodine supplementation.
Another example concerns the simplistic assertion in rich societies that controlling or reducing total fat consumption without changing overall food selection will reduce diseases of affluence. Again there is only weak evidence of benefit, at best. As a consequence of these simplistic strategies, diseases of affluence predominate and costs of health care skyrocket, as in Western countries. One of the most flawed but deeply held assumptions, intentional or otherwise, has been the assertion that overall health will be improved by increasing the consumption of protein, especially that provided by animal-based products. The main supporting evidence cited for this view is that the protein in animal-based foods increases childhood growth and improves resistance to infectious diseases (i.e., improves the immune system). This is a rather narrow interpretation of the evidence that often ignores the simultaneous contributions of improved sanitation and more total food availability.
In contrast, there now is overwhelming evidence that shifting to a diet rich in animal-based protein also directly associates with and, indeed, is causal of the diseases of affluence, especially when accompanied with decreased consumption of whole plant-based foods. In short, many of the arguments used to amend diets for good effect are focused on the addition or subtraction of single nutrients or single nutrient groups. This occurs for diets typically used both in poor and in rich societies.
Arguments that increased protein consumption in poor societies or, conversely, decreased fat consumption in rich societies will improve health are examples of macronutrient changes having very limited effects. It is also hypothesized that increased consumption of specific micronutrients, both in rich and poor societies, will produce health benefits. This type of strategy for health improvement is highly simplistic and problematic. It ignores the health effects associated with the truly major diet differences that distinguish rich and poor societies.
Examples of these differences include either the relative amounts of animal and plant-based foods and/or the relative amounts of highly processed food products rich in fat, salt and sugar. These diet differences, not the single nutrient amendments, are those that primarily differentiate health outcomes observed between rich and poor societies.
Understanding the relative health effects of major and minor diet transitions requires a more sophisticated understanding of nutritional biology. Nutrition is not the consequence of simple, linear biologic effects. Rather, it represents a highly integrated and complex interplay of countless food factors operating upon digestion, absorption and metabolism, within a highly dynamic biological process in the body that optimizes health. This does not lend itself to the solving of health outcomes by simple strategies. An illustration of this type of analysis as it emerged for me is shown in the following sequence of slides and their accompanying notes.
Fortunately, data for much of this illustration were obtained in a national survey of diet, lifestyle and disease mortality characteristics in rural China conducted in the 1980s (Chen et al, 1990). The interpretation of some of the results of this survey, together with a consideration of other findings both before and after the survey, was recently published in a trade book (Campbell and Campbell 2005). Of particular interest to this discussion were the findings of the diet and disease associations in China that showed a causal and ecologic distinction between diseases of poverty and the emerging diseases of affluence in the more urbanized areas of the country (Campbell et al. 1990, Campbell et al. 1992).
Bibliography:
Chen, J., Campbell, T. C., Li, 3. and Peto, R. 1990. Diet, life-style and mortality in China. A study of the characteristics of 65 Chinese counties. Oxford, UK; Ithaca, NY; Beijing, PRC: Oxford University Press; Cornell University Press; People’s Medical Publishing House.
Campbell, T. C., Campbell, T. M., II. 2005. The China Study, Startling Implications for Diet, Weight Loss, and Long-Term Health. Dallas, TX: BenBella Books, Inc.
Campbell, T. C., Chen, 3., Brun, T. et al. 1990. Can developing nations avoid the diseases of affluence? The case in China. In: Brun, T. and Latham, M. (eds). World food issues. Vol 2. Ithaca, NY: Center for the Analysis of World Food Issues, Program in International Agriculture; 56-63.
Campbell, T. C., Chen, 3., Brun, T. et al. 1992. China: from diseases of poverty to diseases of affluence. Policy implications of the epidemiological transition. Ecol. Food Nutr. 27:133-144.
Presented at the European Action on Global Life Sciences conference, September 2007



Comments