


Around 1 percent of the world’s population have the serious neurological condition epilepsy, that is characterized by frequent seizures. While drugs treatments are available for the majority of people with epilepsy, 20 to 30 percent do not respond to medications.
The ability to detect subtle brain abnormalities which cause epileptic seizures may lead to surgical help for those who don't respond to medicine. FCDs are areas of the brain that have developed abnormally and often cause drug-resistant epilepsy. It is typically treated with surgery, however identifying the lesions from an MRI is an ongoing challenge for clinicians, as MRI scans in FCDs can look normal.
TThe team quantified cortical features from the MRI scans, such as how thick or folded the cortex/brain surface was, and used around 300,000 locations across the brain. They then trained the algorithm on examples labelled by expert radiologists as either being a healthy brain or having FCD – dependant on their patterns and features.
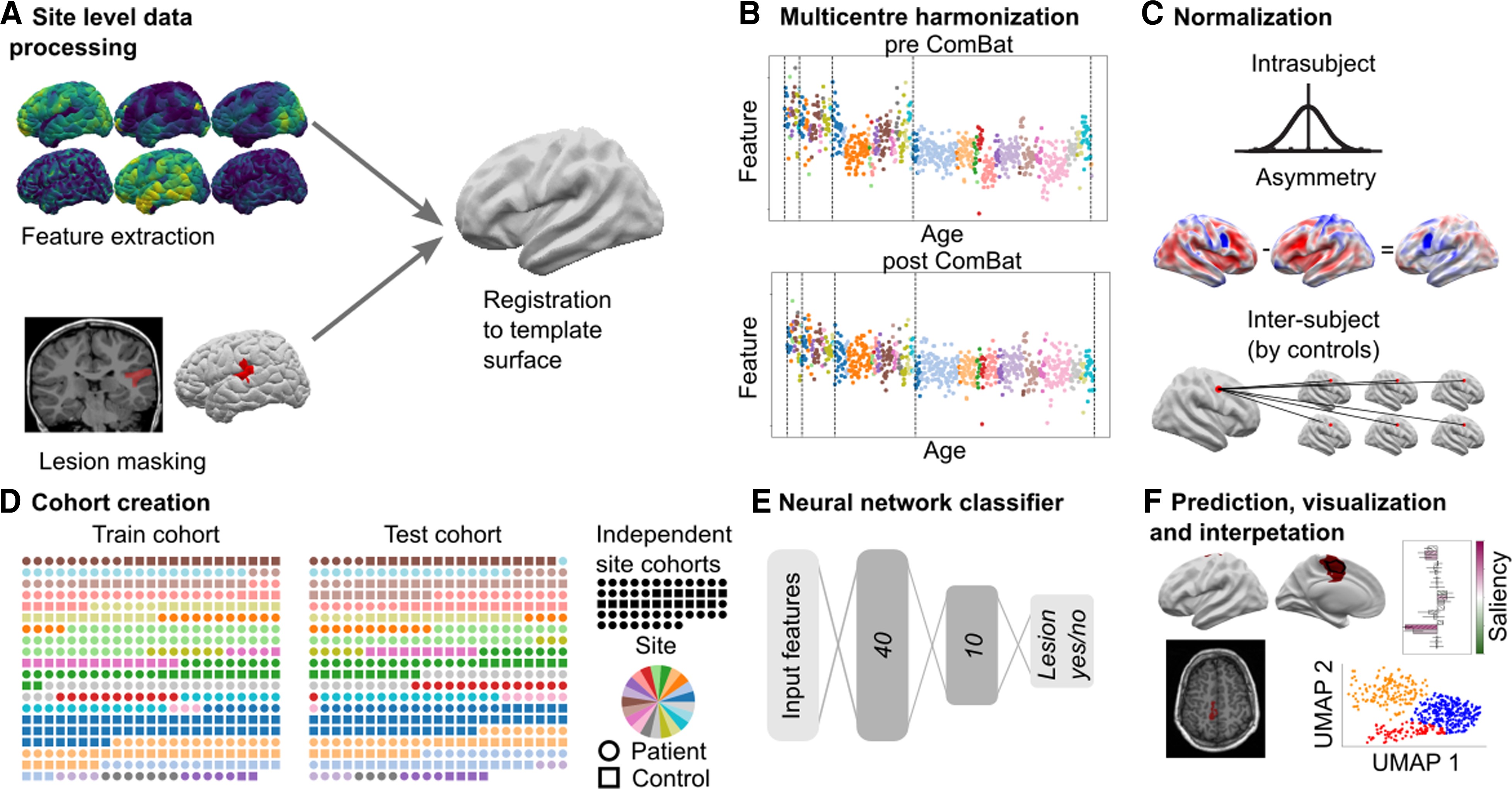
MELD processing pipeline. (A) Local sites extract surface-based morphological features from structural T1 and FLAIR MRI, along with manually delineated lesion masks. These were coregistered to a symmetric template surface and anonymized data matrices are shared with the MELD team. (B) Central preprocessing: the MELD team carried out outlier detection and data harmonization to minimize interscanner feature differences. (C) Morphological features underwent intrasubject, interhemispheric and intersubject normalization. (D) The full cohort was randomly subdivided 50:50 into training/validation cohorts and withheld test cohort. To avoid overfitting, all optimization experiments were carried out on the training/validation cohort prior to final testing on the test cohort and new site cohorts. (E) The neural network classifier was trained to identify lesional vertices from MRI features. Vertex-wise predictions were collected into connected clusters. (F) Classifier predictions mapped to cortical surfaces, lesional features and their relative saliency were plotted; lesional features across the cohort were analyzed.
The findings, published in Brain, found that overall the algorithm was able to detect the FCD in 67 percent of cases in the cohort (538 participants). Yet 178 of the participants had been considered MRI negative, which means that radiologists had been unable to find the abnormality. The MELD algorithm was able to identify the FCD in 63 percent of those cases.
If doctors can find the abnormality in the brain scan, then surgery to remove it can provide a cure. In children who have had surgery to control their epilepsy, FCD is the most common cause, and in adults it is the third most common cause. Additionally, of patients who have epilepsy that have an abnormality in the brain that cannot be found on MRI scans, FCD is the most common cause.
The MELD FCD classifier tool can be run on any patient with a suspicion of having an FCD who is over the age of 3 years and has an MRI scan.



Comments