


A new article suggests paying them. It is not that rural doctors are bad, there just are not enough. In a heavily-regulated, high-tax, litigation-run state like California, it is hard for rural doctors to charge affordable prices and stay in business. Inability to create a product your neighbors can afford is not exclusive to doctors. America has high prescription drug costs because people want the best, and early adoption means higher expenses, which means high purchase costs, and with profit margins here drug companies can charge less wealthy nations such as Canada a reduced amount and still be profitable.
That model may work for medical care also. A wealthy doctor in Pacific Heights is making enough money they can afford to travel to rural areas for less.There is no social currency in that, though. Urban people often look down on rural communities but feel positively about poor people in other countries. So you'd have to pay them in a way you wouldn't if they were going overseas to work for a French-sounding doctor group that pretends it's only about medicine.
The authors get some things right and some things wrong. They note higher death rates from coronary heart disease in rural areas is due to a lack of cardiologists. More cardiologists won't reduce heart disease, hypertension, and stroke, better lifestyle and medicine do. There is no lack of awareness in 2024. If we care about 60,000,000 Americans at elevated risk of early death linked to those issues the solution is to make blood pressure medication as easy to get online as viagra. Rural people, especially in California, face long wait times for an appointment, the internet is the obvious solution for people who already have a diagnosis. A specialist giving them meaningless advice like 'eat less salt' because they read an epidemiology paper isn't saving anyone.
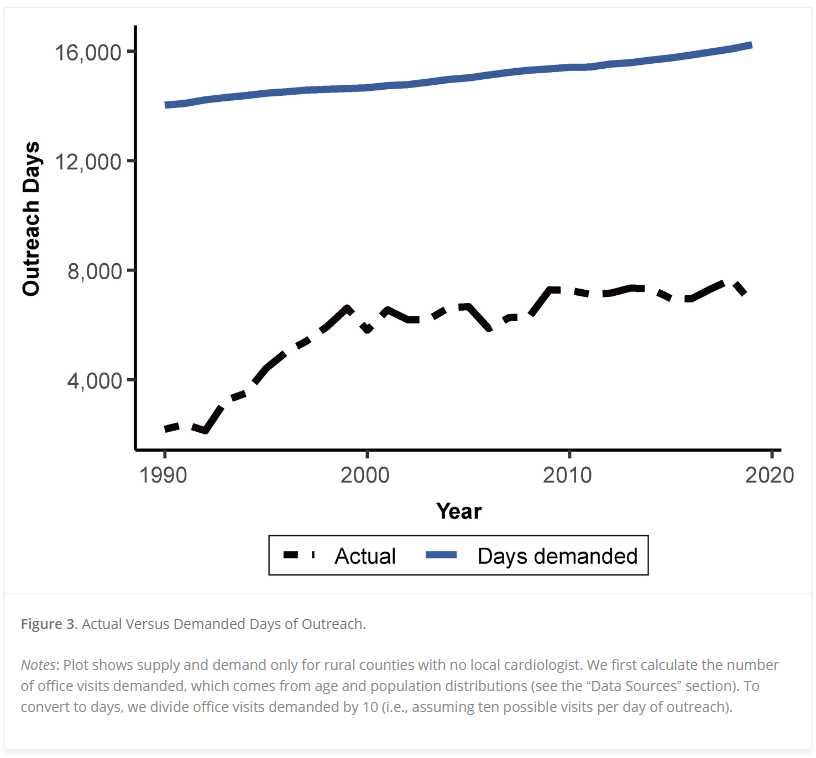
Yet because cardiologists are specialists and clustered in wealthy urban areas, they might be inclined to visit rural areas without the sacrifice primary care doctors have to make to help poor communities. The authors use Idaho in their example, noting there are 10.6 cardiologists per 100,000 people in dense areas but only 1.5 in rural ones. For specialists that makes sense; you want to see as many people as possible, but it also means that if they were paid and a schedule was created in advance, where rural people could get appointments in that same time density, cardiologists might be inclined to travel a short way.
The big issue, especially in California, will be enough primary care once politicians make health care free for illegal immigrants. It is already expensive for those who pay, while those on the Affordable Care Act plans often find no available openings when they disclose that is their insurance plan.


Comments